
More Information
Submitted: December 24, 2024 | Approved: January 03, 2025 | Published: January 06, 2025
How to cite this article: Saini K, Sharma P, Sharma B, Dubey AK, Bhatnoo M, Thakur P, et al. Drug Rehabilitation Centre-based Survey on Drug Dependence in District Shimla Himachal Pradesh. J Addict Ther Res. 2025; 9(1): 001-006. Available from: https://dx.doi.org/10.29328/journal.jatr.1001032
DOI: 10.29328/journal.jatr.1001032
Copyright License: © 2025 Saini K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: The rehabilitation centre; Drug dependency; Cross-sectional survey; Demographic data; Drug history

Drug Rehabilitation Centre-based Survey on Drug Dependence in District Shimla Himachal Pradesh
Kanishka Saini, Palak Sharma, Bhawna Sharma *, Atul Kumar Dubey, Muskan Bhatnoo, Prajkta Thakur, Vanshika Chandel and Ritika Sinha
*, Atul Kumar Dubey, Muskan Bhatnoo, Prajkta Thakur, Vanshika Chandel and Ritika Sinha
Department of Forensic Science, Alakh Prakash Goyal Shimla University, Shimla, Himachal Pradesh, India
*Address for Correspondence: Bhawna Sharma, Department of Forensic Science, Alakh Prakash Goyal Shimla University, Shimla, Himachal Pradesh, India, Email: bhawnasharma@agu.edu.in
Aim and objective: This study aimed to determine the prevalence and characteristics of drug dependency among patients in various rehabilitation centers in the Shimla district.
Introduction: Drug abuse is a multifaceted and significant issue impacting individuals worldwide, and the city of Shimla in Himachal Pradesh is no exception. Despite its reputation as a picturesque hill station known for its natural beauty and rich cultural heritage, Shimla faces challenges related to substance abuse.
Materials and methods: A cross-sectional survey was conducted, gathering demographic data, drug history, and indicators of dependency from the participants.
Result: The findings revealed that 60% of the patients were drug-dependent, with 44% addicted to heroin and 11% to alcohol. Additionally, 60% of the patients reported a family history of chemical dependency. The study also identified associated psychological disorders such as depression and anxiety, as well as interpersonal and environmental factors like peer pressure and coping mechanisms such as avoidance and denial.
Conclusion: These findings underscore the complexity of drug dependency, highlighting the need for comprehensive, multidimensional approaches to address the medical, emotional, and social aspects of addiction.
Drug abuse is a complex and serious issue affecting people worldwide, and Shimla City, nestled in the picturesque hills of Himachal Pradesh, is no exception. Despite its reputation as a charming hill station known for its natural beauty and rich cultural heritage, Shimla is not immune to substance abuse problems. Beneath its serene exterior lies a growing concern about drug addiction, affecting individuals from all walks of life [1]. Drugs possess an allure that transcends social and geographic boundaries. Like many other cities, Shimla faces high rates of drug misuse among its residents due to various factors [2]. Addiction can result from multiple complex factors, including peer pressure, mental health issues, and the desire to escape life’s challenges. Effective intervention techniques must address not only the symptoms but also the root causes of drug dependence. Our study aims to uncover these underlying determinants [3]. Furthermore, easy access to illegal substances and a lack of awareness about the dangers of substance misuse contribute to Shimla’s high rate of drug dependence. The presence of hidden drug dealers and underground networks makes acquiring drugs alarmingly easy for many community members [4]. The state of Himachal Pradesh has been battling drug problems, particularly with substances like chitta, but the situation seems to worsen each year [5]. Drug abuse has wide-ranging impacts on individuals, families, workplaces, and the broader community. The ripple effects of addiction strain relationships threaten livelihoods and tear apart the social fabric. Thus, combating drug addiction is a societal imperative requiring cooperation from all sectors, not just a matter of personal health [6]. In Shimla, addressing drug dependence requires a multimodal strategy involving treatment, prevention, and rehabilitation initiatives. Prevention programs should focus on raising public awareness about substance addiction’s dangers, promoting positive coping strategies, and building resilience in individuals and communities. Peer support groups, community outreach programs, and school-based initiatives can play crucial roles in deterring drug use and reducing its prevalence [7]. Ensuring access to comprehensive and evidence-based treatment and recovery options for those struggling with drug use is vital. This includes social support services, behavioral therapy, medication-assisted treatment, and counseling. Collaboration among healthcare providers, mental health professionals, social workers, and community organizations is essential to provide holistic care and address the diverse needs of those affected by drug use [8]. However, addressing drug abuse goes beyond service delivery and policy changes; it requires changing societal attitudes toward addiction [9]. Stigma and discrimination associated with substance use disorders can hinder treatment and support. Community-based programs that challenge prejudices, foster empathy, and promote inclusion are necessary to create supportive environments for recovery and rehabilitation [10]. In summary, addressing drug abuse in Shimla city is a complex task that requires a comprehensive, multimodal approach. Through thorough surveys and cross-sector collaboration, the drug rehabilitation center aims to spark discussion, raise public awareness, and secure funding to address this urgent issue [11]. We envision a future where Shimla is resilient against drug abuse, providing a safe and thriving environment for all its residents through shared commitment and coordinated efforts [12]. Ensuring that persons battling drug use have access to thorough and evidence-based treatment and recovery options is also crucial to their support. This covers a variety of interventions, including social support services, behavioral therapy, medication-assisted treatment, and counseling. To provide holistic treatment and meet the various needs of those impacted by drug use, collaboration between healthcare providers, mental health specialists, social workers, and community organizations is essential [13]. But combating drug abuse calls for more than simply service delivery and legislative changes—it also calls for a change in how society views addiction in general [14]. The stigma and discrimination associated with substance use disorders can serve as obstacles to getting treatment and assistance. Thus, developing supportive environments that aid in recovery and rehabilitation requires community-based programs that dispel prejudices, encourage empathy, and promote inclusion in summary; comprehending drug abuse in Shimla City is a challenging task that calls for an all-encompassing, multimodal strategy. Through the implementation of a thorough survey and cross-sector collaboration, the drug rehabilitation center hopes to stimulate discussion, increase public awareness, and secure funding for the resolution of this pressing problem [15].
The rising issue of drug abuse in Shimla City, despite its scenic and tranquil image, has become a growing concern that demands urgent attention. This publication is of significant interest as it addresses a critical yet often overlooked aspect of the city’s socio-economic landscape—substance abuse and its complex socio-cultural dynamics. Shimla, known for its natural beauty, has been increasingly affected by drug addiction, particularly with substances like chitta, which have become easily accessible due to hidden underground networks. This study explores not only the root causes of addiction in the region but also highlights the urgency of adopting a comprehensive, multimodal approach to tackling the problem, integrating prevention, treatment, and rehabilitation strategies. The paper presents valuable insights into the role of community-based programs, peer support groups, and school-based initiatives in reducing drug abuse rates. Moreover, it underscores the importance of challenging societal stigma and fostering a more inclusive, empathetic approach toward those affected by addiction. The findings of this study are relevant not only for Shimla but also for similar hill stations and urban areas grappling with the growing menace of drug misuse. In calling for cross-sector collaboration, this publication aims to stimulate public awareness, inform policy, and encourage funding for long-term solutions. Ultimately, the research seeks to create a blueprint for other regions battling drug abuse, making it a timely and impactful contribution to the discourse on substance use and public health. The present study aims at surveying to spark discussion and raise awareness about the extent and kind of drug. We picture a future in which Shimla City emerges resilient against the plague of drug use, providing a secure and thriving environment for all its citizens, through shared commitment and coordinated effort [16].
In the present study, a questionnaire [17] was prepared that covered aspects such as the type of drugs used, and frequency of usage [18]. Initiation of the drug use, the reason for usage, barriers to seeking treatment, and perceptions of available services [Drug Use Questionnaire (DAST-20)] [17]. Literature has been thoroughly investigated that is currently available on drug dependency in Shimla. Government publications, scholarly research, and regional health data may all fall into this category [18]. A survey tool has been developed to gather pertinent data on drug abuse in the district of Shimla, Himachal Pradesh. A questionnaire covering aspects such as the types of drugs used, frequency of usage, initiation into drug use, reasons for usage, barriers to seeking treatment, and perceptions of available services was prepared. The survey was conducted through visits to rehabilitation centers as shown in Table 1 where information was gathered from patients and owners using the prepared questionnaire. In-person interviews were employed to administer the survey, ensuring privacy and anonymity to encourage honest responses.
| Table 1: Rehabilitation Centres Visited. | |||
| S.no. | Rehabilitation Centre | No. of Participants | Location |
| 1. | Care And Concern Foundation De-Addiction Rehabilitation Centre Shimla | 14 | Village New Majhar, Junga Road, Beolia, Shimla - 171009 (Near Thakur Bhojnalaya) |
| 2. | Sunrise rebirth foundation | 20 | Vill, Panog, Shoghi, Himachal Pradesh 171009 |
| 3. | Revive life foundation | 30 | Chandel building, near Rohrudhaba, Kholgali, Theog, Himachal Pradesh 171201 |
After data collection, a comprehensive report was compiled to conduct further analysis, aiming to identify significant patterns and insights regarding drug abuse. It was carried out using the simple percentage method where parameters like characteristics of the respondents and patterns of drug abuse were investigated. Additionally, data was graphically represented using bar charts to enhance visual clarity and interpretation.
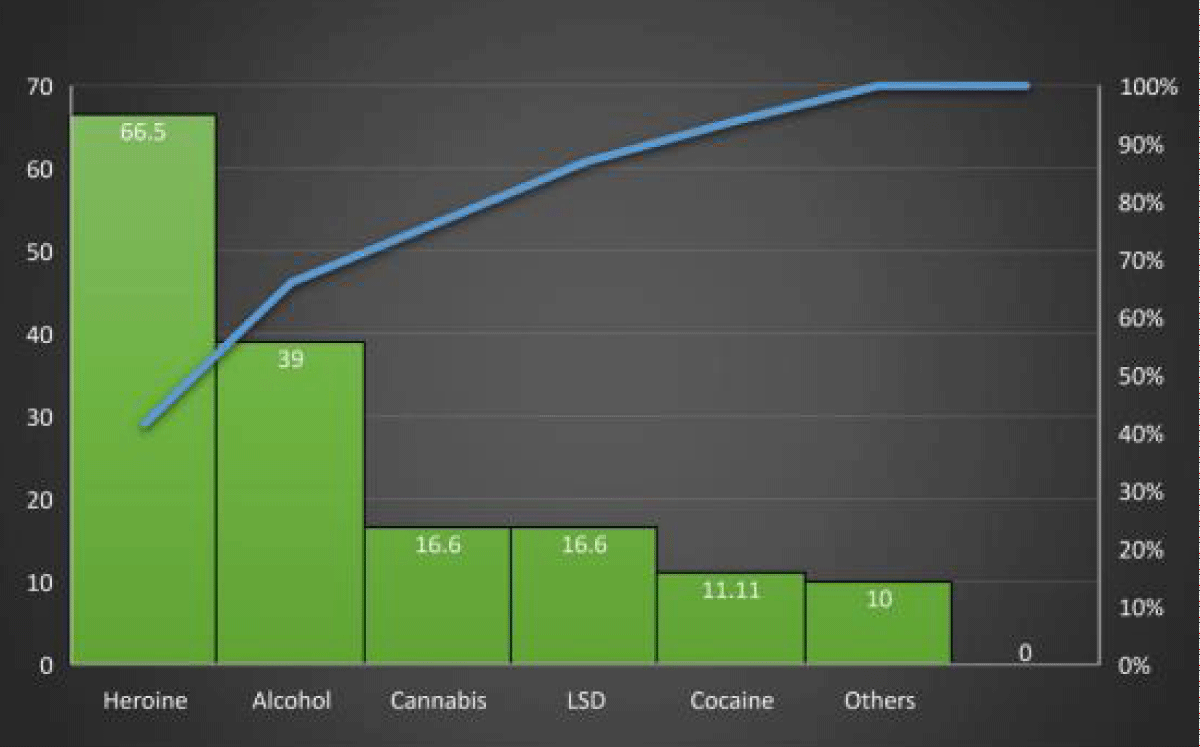
Figure 1: Inclusion Criteria of Respondents.
In the present study, a survey has been conducted in the district of Shimla, Himachal Pradesh rehabilitation centers. The aim was to gather pertinent data on drug abuse patterns and it was carried out using a questionnaire. The characteristics of respondents in the present study, 18 volunteers participated with a 100% response rate. The characteristics of the respondents are summarized in Tables 1-4. It revealed that a significant number of male addicts, which was one-third of the whole sample (33.33%), were admitted to the drug rehabilitation centers. The highest concentration of drug addicts was between the ages of 20 and 25 (27.78%), followed by 15-20 (16.667%). Almost one-sixth (16.67%) of the addicts were between the ages of 20 and 25 (Figure 1). The highest number of drug addicts had graduated with an above-average level of educational qualification. Most of the addicts were students (61%), and over two-thirds of the respondents (40.66%) did not know the harmful impact of drug addictions. The drug abuse patterns survey questionnaire comprehensively covered multiple facets, encompassing types of drugs used, frequency of usage, initiation into drug use, reasons for usage, barriers to seeking treatment, and perceptions of available services. From this dataset, deductive conclusions were drawn as shown in Table 2. The findings indicated that the most common type of drug used by the sample of addicts was heroin (61.11%). Alcohol and cocaine were the least popular drugs among the studied sample (11.11%). One-third of the addicts (30%) were dependent on family for their drug expenditure. A family problem was the main reason (70%) for getting involved with drug addiction, followed by frustration among the respondents due to different reasons. Nearly half of the respondents got involved with drug addiction, followed by enjoyment and fun purposes with friends. Heroin was the most common first drug of abuse in the combined sample, with a share of (61%), followed by alcohol (50%), cannabis (22%), LSD (11%), cocaine (11%), and other drugs. 50% years of regular use. Many of the people interviewed in Shimla had been using drugs for five years or more as shown in Table 2. Additionally, data was graphically represented using bar charts to enhance visual clarity and interpretation shown in Figure 2.
| Table 2: Prevalence of Drugs. | ||
| Types of Drugs | Total | Percentage |
| Heroin | 11 | 61.11% |
| Alcohol | 9 | 50% |
| Cannabis | 4 | 22.22% |
| LSD | 2 | 11.11% |
| Cocaine | 2 | 11.11% |
| Others | 9 | 50% |
| Total | 18 | 100% |
| Table 3: Inclusion Criteria of Respondents (Gender). | ||
| Characteristics of the Respondents | Total No. of Sample | Percentage of Respondents |
| Male | 18 | 100% |
| Female | 18 | 100% |
| Table 4: Inclusion Criteria of Respondents (Age/Year) Composition. | ||
| Characteristics of the Respondents (Years) | Total No. of Sample | Respondents (%) |
| 15-20 years | 3 | 16.66% |
| 20-25 years | 5 | 27.78% |
| 25-30 years | 3 | 16.66% |
| 30-35 years | 2 | 11.11% |
| 35-40 years | 2 | 11.11% |
| 40-45 years | 0 | 0% |
| 45-50 years | 1 | 5.5% |
| 50-55 years | 1 | 5.5% |
| 55-60 years | 1 | 5.5% |
| Total | 18 | 100% |
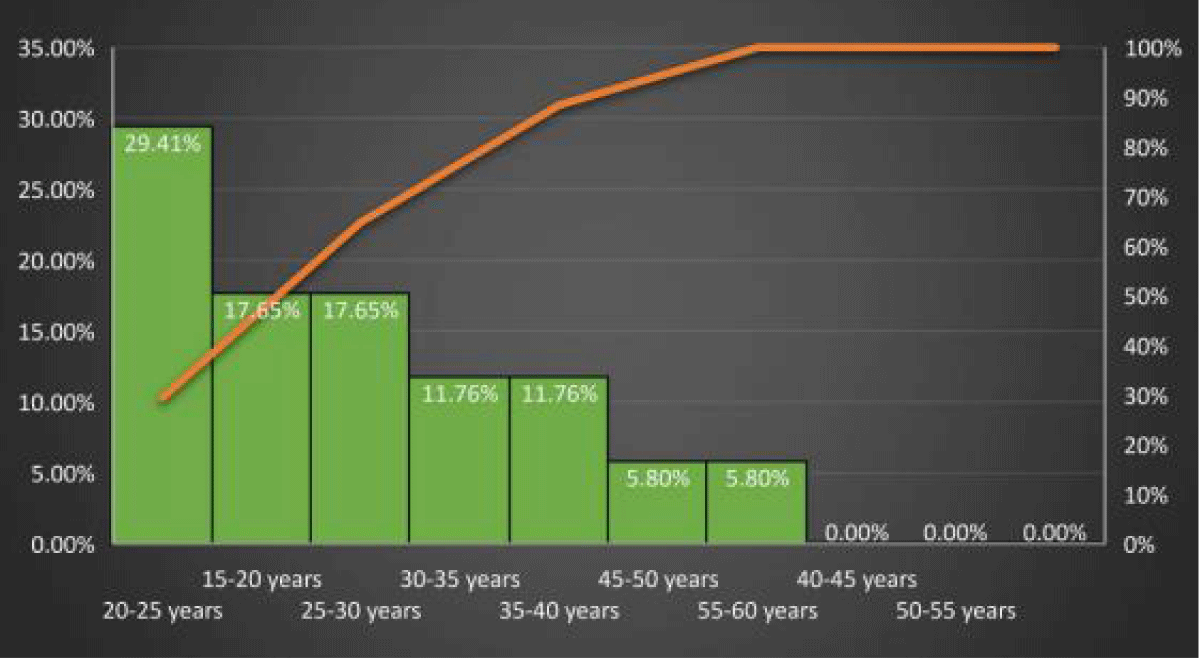
Figure 2: Prevalence of Drugs.
The current study highlights that most addicts in district Shimla have initiated drug use at a young age. This trend mirrors findings from the present study, where approximately 80% of drug addicts were adolescents and young men aged 15 to 30 years. Recent reports from local newspapers further emphasize that a significant number of drug-addicted individuals in Shimla fall within the 18 to 30-year-old age bracket, indicating widespread drug availability and insufficient law enforcement oversight, posing risks for future generations [19]. Heroin emerges as the most abused drug among the surveyed addicts, alongside cannabis and alcohol. Alcohol’s prevalence is attributed to its easy accessibility and societal acceptance, while the increasing use of cannabis may reflect shifting perceptions regarding its risks and legal status. Substance abuse spans various age groups but is particularly pronounced among individuals aged 20 to 30, who contend with pressures from social, professional, and academic environments [20]. These findings underscore the urgent need for targeted interventions tailored to address the specific challenges faced by this demographic. Moving forward, regular surveys, stakeholder engagement, and data-driven strategies are essential for developing effective policies and programs aimed at combating substance abuse in Shimla district, Himachal Pradesh [21].
Recommendations and future directions
While the government periodically conducts surveys to assess drug abuse patterns, no up-to-date survey is available for the present year, i.e. 2024 in Shimla district, Himachal Pradesh. This study underscores the necessity for a comprehensive survey to gain a precise understanding of drug abuse in the Shimla district. Rigorous analysis of survey findings will identify emerging trends, high-risk populations, and geographical hotspots, informing targeted interventions. Detailed reports will guide the development of evidence-based strategies tailored to specific needs. Additionally, qualitative research focusing on psychological profiling and cultural influences will provide deeper insights into individual experiences, motivations, and challenges in rehabilitation. Exploring ethnicity and regional factors will further enhance intervention effectiveness by addressing cultural beliefs, social networks, and environmental influences. Such a study can also be expanded to other districts and states and a comparative analysis can be carried out. Integrating both quantitative and qualitative research methodologies is crucial for advancing our understanding and refining drug rehabilitation efforts [22]. This study has several limitations that must be considered while interpreting the findings. First, the sample size was relatively small, comprising only participants from three rehabilitation centers, which may not fully represent the broader population of drug users in the Shimla district. Second, the reliance on self-reported data introduces the possibility of bias, as participants may underreport or overreport certain behaviors due to stigma or memory recall issues. Third, this study primarily focused on quantitative data, limiting the depth of understanding of the psychological, cultural, and social contexts of addiction. Finally, the cross-sectional nature of the study does not allow for the assessment of causal relationships or long-term trends in drug dependency. From the authors’ perspective, the findings of this study highlight the urgent need for holistic and evidence-based approaches to tackle the drug abuse epidemic in Shimla. While the study identifies key patterns and contributors to substance dependency, it also underscores the importance of addressing underlying societal factors, such as unemployment, peer influence, and familial discord, through policy and community-level interventions. The authors believe that a multidisciplinary approach, combining healthcare, education, and social work, is essential to fostering resilience and reducing the prevalence of substance abuse. Additionally, there is a pressing need to destigmatize addiction to encourage individuals to seek help without fear of judgment. Future studies should improve the approach to data gathering and processing, using technology in remote assistance, and fostering collaboration to build a patient community. Holistic, culturally appropriate, and gender-sensitive interventions are critical to meet the complex requirements of persons experiencing drug dependence and to support recovery [23].
Drug dependency remains a critical issue across India, affecting individuals from diverse backgrounds. While studies in different regions of the country offer valuable insights into the patterns and impacts of addiction, a comparative approach can help identify commonalities and regional differences [24-30]. The present study in Shimla contributes to the growing body of research on drug dependency, focusing on local factors that influence addiction. The current study sheds light on the prevalence of heroin and alcohol abuse among patients in rehabilitation centers, in District Shimla, with a notable influence of familial substance dependency and psychological disorders like depression and anxiety. 60% of participants reported a family history of chemical dependency, emphasizing the intergenerational nature of addiction, and a significant number of participants were struggling with psychological challenges, which contributed to their addiction. In terms of treatment, the study also highlighted the demand for community-based interventions and enhanced mental health services.
When compared with the National Survey on Extent, pattern, and Trends of Drug Abuse in India [31] which encompasses a broader range of regions, it becomes evident that while certain patterns are shared, others are unique to specific locales.
The Rapid Assessment Survey, covering both urban and rural areas, highlighted heroin as the dominant substance in metropolitan cities like Delhi, Kolkata, and Mumbai (71%), aligning with Shimla’s findings. However, in other non-metropolitan areas, cannabis use was much more prevalent, accounting for 22% of users, whereas Shimla did not report cannabis as a major concern. Additionally, the RAS noted the high use of injectables (especially heroin and buprenorphine), with 43% of users reporting injecting drug use, a factor that was not as prominent in Shimla’s findings, suggesting either a lower prevalence of injectable drug use or possible underreporting in the current study.
The psychological factors observed in Shimla align with the RAS’s finding that many drug users across different states also exhibit depression, anxiety, and other mental health disorders. However, the RAS study placed additional focus on high-risk behaviors such as unsafe sex, particularly with sex workers, and the associated risks of HIV, which was a less emphasized issue in the Shimla study. While Shimla highlighted coping mechanisms such as avoidance and denial, the RAS emphasized behavioral risks, such as unsafe sex and needle sharing, which are closely tied to the transmission of infectious diseases, especially in areas with high injectable drug use.
Treatment gaps are a shared challenge. In Shimla, there was a marked need for more comprehensive treatment options, including mental health support and family-based interventions. Similarly, the RAS report noted the lack of substitution therapies, harm reduction programs, and adequate rehabilitation facilities to meet the growing demand. While the RAS focused more on harm reduction strategies for injectors and the general population, the present study suggested a more localized approach, focusing on community outreach and integrating addiction treatment with mental health services.
In conclusion, while the study in Shimla and the RAS share several common findings, such as the dominance of heroin abuse and the mental health challenges associated with addiction, their differences highlight the regional nuances of drug use patterns and the specific needs of each area. The Shimla study adds depth by emphasizing familial and psychological influences on drug use, while the RAS offers a broader, national perspective, incorporating a wider range of substances and risk behaviors, such as injectable drug use and HIV transmission. Both underscore the urgent need for a multidimensional approach to drug dependency, tailored to local contexts but informed by national data to ensure that interventions are both effective and appropriate.
The study discusses the complex issue of drug dependence among patients, with a focus on the interaction of drug use, mental condition, and social environment in a rehabilitation centre. Considering the high rates heroin and alcohol consumption and the strong connection between substance use, mental disorders, and social factors. It was revealed that a significant number of male addicts, and the highest concentration of drug addicts were between the ages of 20 and 25 (27.78%), followed by 15-20 (16.667%). Almost one-sixth (16.67%) of the addicts were between the ages of 20 and 25. Their primary motivation for using drugs initially stemmed from the desire to experience pleasure or to witness their friends’ using drugs. Over time, repeated use led to the development of a drug-taking habit. It is crucial to develop a multi-faceted approach to intervention. It means that the rehabilitation process should address not only the somatic aspect of addiction but also offer significant support in addressing mental disorders and social adaptation processes.
- Bhat SA, Imtiaz N. Drug addiction in Kashmir: issues and challenges. J Drug Abuse. 2017;3(3). Available from: https://doi.org/10.21767/2471-853x.100059
- Efferth A. Development of drug resistance in Trypanosoma brucei rhodesiense and Trypanosoma brucei gambiense. Treatment of human African trypanosomiasis with natural products (Review). Int J Mol Med. 1998;22(4):411-9. Available from: https://pubmed.ncbi.nlm.nih.gov/18813846/
- Hasan M, Shahin A. Drug rehabilitation center based survey on drug dependence in Dhaka City. Updat Dent Coll J. 2013;3(1):32-6. Available from: https://pdfs.semanticscholar.org/d657/ba24afb345337eb0a341a9f240a9071b389a.pdf
- Shende H, Holey S. Formulating design guidelines for drug de-addiction center in India. Int J Res Eng Sci Manag. 2024;7(4):109-14. Available from: https://journal.ijresm.com/index.php/ijresm/article/view/3004
- Ibrahim F, Kumar N. Factors affecting drug relapse in Malaysia: An empirical evidence. Asian Soc Sci. 2009;5(12):37-42. Available from: https://doi.org/10.5539/ass.v5n12p37
- Joshi U, Kadri A, Bhojiya S. Prevention of parent to child transmission services and interventions - coverage and utilization: A cohort analysis in Gujarat, India. Indian J Sex Transm Dis AIDS. 2010;31(2):92-8. Available from: https://doi.org/10.4103/0253-7184.74983
- Kaplan HB, Meyerowitz JH. The community’s response to substance misuse: evaluation of a halfway house: integrated community approach in the rehabilitation of narcotic addicts. Int J Addict. 1969;4(1):65-76. Available from: https://doi.org/10.3109/10826086909062002
- Rai S, Kumar G, Avinash Jnaneswar S, Vinay Jha K, Singh A. Substance use and oral health sensations among substance users residing in rehabilitation centres in an Indian city. Indian J Dent Res. 2022;33(1):7-13. Available from: https://doi.org/10.4103/ijdr.ijdr_213_20
- Ramakrishnan T, Ezhumalai S, Ramasamy D. Profile of psychosocial rehabilitation centres for persons with substance use disorders in Bengaluru: a cross-sectional study. J Psychosoc Rehabil Ment Health. 2022;29:293-302. Available from: https://doi.org/10.1007/s40737-022-00265-9
- Thakur MS, Anupama K. Assess the lived experiences and quality of life in substance abuse patients admitted to de-addiction centres of Himachal Pradesh and Punjab. J ReAttach Ther Dev Divers. 2023;6(1):992-1002. Available from: https://doi.org/10.53555/jrtdd.v6i1.2548
- Al-Khateeb W. Demographics of drug addicts of Al-Sadiq Al-Taieb Association in Bethany. J Posit Psychol Wellbeing. 2022;6(1):3822-3849. Available from: http://184.168.115.16/index.php/jppw/article/view/6246
- Alaghemandan H, Ghaffari Darab M, Khorasani E, Namazi E, Maniyan MH, Barati M. Personality traits and their relationship to demographic features in addicts referring to a drug rehabilitation center in the city of Isfahan, Iran. Iran J Public Health. 2015;44(4):551. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4441968/
- Giang LM, Trang NT, Hoe HD, Anh NH, Thanh T, Bart G. “If they get out of drug rehab centers, they’re on their own”: Opportunities and challenges for people released from compulsory drug rehabilitation centers to communities in Vietnam. Int J Drug Policy. 2024;128:104443. Available from: https://doi.org/10.1016/j.drugpo.2024.104443
- Maehira Y, Chowdhury E, Reza M, Drahozal R, Gayen T, Masud I, et al. Factors associated with relapse into drug use among male and female attendees of a three-month drug detoxification–rehabilitation programme in Dhaka, Bangladesh: a prospective cohort study. Harm Reduct J. 2013;10(1):14. Available from: https://doi.org/10.1186/1477-7517-10-14
- Mehra MR, Canter CE, Hannan MM, Semigran MJ, Uber PA, Baran DA, et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. J Heart Lung Transplant. 2016;35(1):123. Available from: https://doi.org/10.1016/j.healun.2015.10.023
- Parmar P. Knowledge and awareness regarding substance addiction among medical students of Valsad, Gujarat. Forensic Sci Addict Res. 2018;4(1). Available from: https://doi.org/10.31031/fsar.2018.04.000585
- United Nations Office on Drugs and Crime (UNODC). Drug report 2023. Available from: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html
- Drug Abuse Screening Test (DAST-20). (n.d.). Available from: https://adai.uw.edu/instruments/pdf/Drug_Abuse_Screening_Test_105.pdf
- R NS, Lukman ZM. Assessing the recovery levels of drug addicts in rehabilitation centers using drug addiction recovery instruments. Asian People J (APJ). 2023;6(2):180-187. Available from: https://doi.org/10.37231/apj.2023.6.2.414
- Rawat N, Sharma A. De-addiction of the addicted through education. In: Routledge EBooks. 2023:171-185. Available from: https://doi.org/10.4324/9781003370222-17
- Sharifi H, Kharaghani R, Sigari S, Emami H, Sadr M, Masjedi MR. Common methods to treat addiction in treatment-rehabilitation centers in Tehran. Iran J Public Health. 2012;41(4):63-8. Available from: https://pubmed.ncbi.nlm.nih.gov/23113166/
- When treatment is violence: making, treating, and regulating addiction in Nepali private rehabilitation centers. ProQuest. 2019.
- Sharma B, Arora A, Singh K, Singh H, Kaur P. Drug abuse: Uncovering the burden in rural Punjab. J Family Med Prim Care. 2017;6(3):558-62. Available from: https://doi.org/10.4103/2249-4863.222037
- Singh R (Col). Be aware of drugs. 2nd ed. Talwandi Sabo, Punjab: AKAL UNIVERSITY; 2022.
- United Nations Office on Drugs and Crime (UNODC). Online world drug report 2023 - Latest data and trend analysis. Available from: https://www.unodc.org/unodc/en/data-and-analysis/wdr-2023-online-segment.html
- Substance abuse and addiction statistics [Internet]. 2023 [cited 2023 Aug 31].
- Forchuk C, Serrato J, Scott L. People with lived and living experience of methamphetamine use and admission to hospital: what harm reduction do they suggest needs to be addressed? Health Promot Chronic Dis Prev Can. 2023;43(6):338-47. Available from: https://doi.org/10.24095/hpcdp.43.7.04
- Temane A, Rikhotso T, Poggenpoel M, Myburgh C. Adolescents' lived experiences of substance abuse in the Greater Giyani Municipality. Curationis. 2023;46(1):e1-e9. Available from: https://doi.org/10.4102/curationis.v46i1.2379
- Ates N, Unubol B, Bestepe EE, Bilici R. The effect of perceived social support on quality of life in Turkish men with alcohol, opiate and cannabis use disorder. J Ethn Subst Abuse. 2023;22(2):316-36. Available from: https://doi.org/10.1080/15332640.2019.1685051
- Simirea M, Baumann C, Bisch M, Rousseau H, Di Patrizio P, Viennet S, et al. Health-related quality of life in outpatients with substance use disorder: evolution over time and associated factors. Health Qual Life Outcomes. 2022;20(1):26. Available from: https://doi.org/10.1186/s12955-022-01935-9
- United Nations International Drug Control Programme, Regional Office for South Asia, & Ministry of Social Justice and Empowerment, Government of India. Rapid assessment survey of drug abuse in India. New Delhi: UNDCP, ROSA. Available from: https://www.unodc.org/pdf/india/RAS.pdf